Celiac Disease is a serious, hereditary autoimmune disorder where the ingestion of gluten, a protein found in wheat, barley, and rye, leads to damage in the small intestine. Unlike a food allergy, which causes an immediate inflammatory response, Celiac Disease triggers the immune system to attack the body’s own healthy tissue, specifically the villi that line the small intestine. This damage results in malabsorption of vital nutrients, leading to a wide range of symptoms from digestive distress to neurological issues.
Currently, the only treatment is a strict, lifelong gluten free diet. Early diagnosis and meticulous management are essential to preventing long-term complications such as osteoporosis, infertility, and secondary autoimmune conditions.

Understanding the Autoimmune Connection
Celiac Disease is often misunderstood as a “lifestyle choice” or a simple food intolerance. In reality, it is a complex autoimmune condition that affects approximately 1 in 100 people worldwide. When an individual with Celiac Disease consumes gluten, their immune system perceives the gliadin and glutenin proteins as foreign invaders. Instead of just attacking the gluten, the immune response mistakenly targets the villi—tiny, finger-like projections lining the small intestine.
The villi are responsible for absorbing every nutrient, vitamin, and mineral from the food we eat. When they become flattened or destroyed (a process known as villous atrophy), the body can no longer absorb nutrition effectively, regardless of how healthy the diet may be. This “malabsorption” is the root cause of the diverse and often debilitating symptoms associated with the disease.

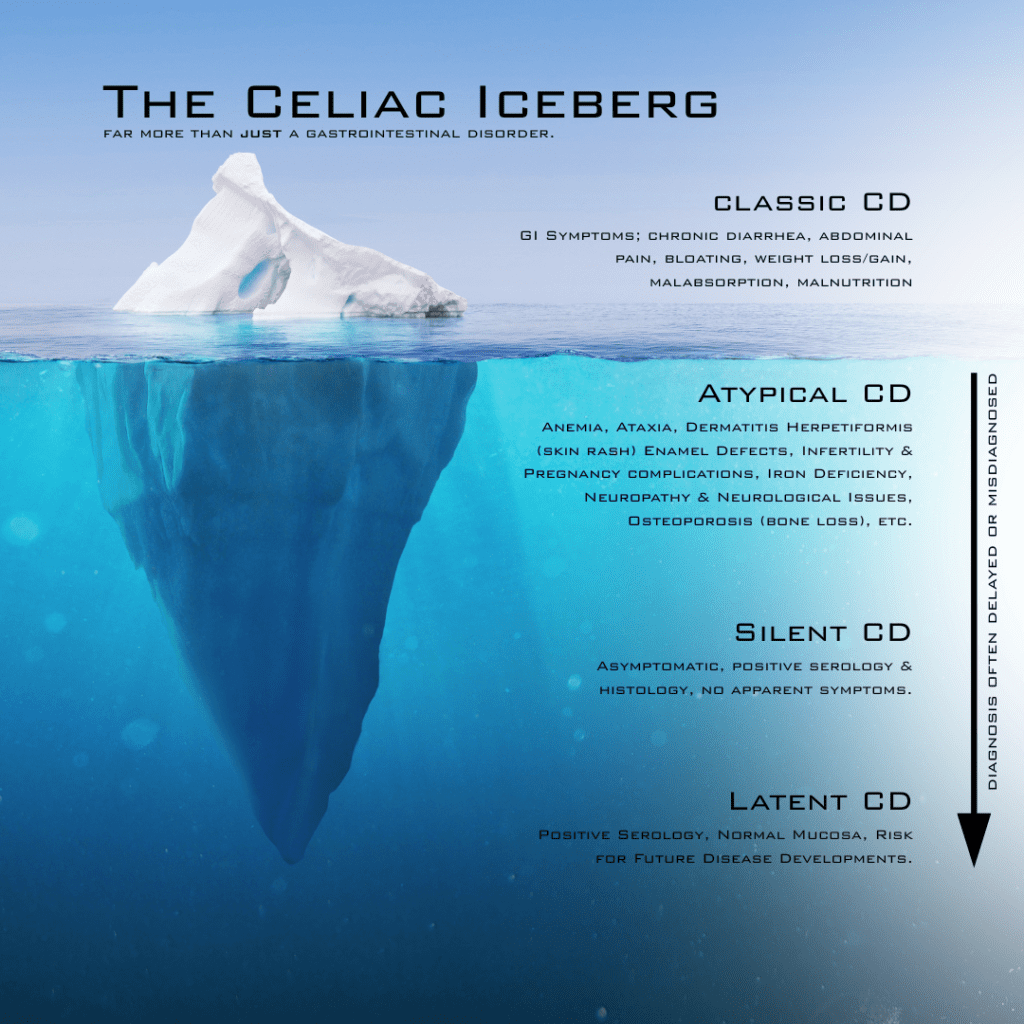
The “Chameleon” Disease: Identifying Symptoms
Celiac Disease is famously called a “chameleon” because its symptoms vary significantly between individuals. Some people experience classic gastrointestinal issues, while others present with “silent” symptoms that seem entirely unrelated to the gut.
Classical Symptoms:
- Chronic Diarrhea or Constipation: Often alternating or persistent.
- Abdominal Pain and Bloating: Frequently misdiagnosed as Irritable Bowel Syndrome (IBS).
- Weight Loss: Though notably, many adults with Celiac are actually overweight at the time of diagnosis.
- Malodorous or Fatty Stools: Indicative of fat malabsorption.
Non-Classical (Extra-Intestinal) Symptoms:
- Iron-Deficiency Anemia: Often the only sign in adults, unresponsive to supplements.
- Chronic Fatigue and “Brain Fog”: A persistent feeling of exhaustion or cognitive cloudiness.
- Dermatitis Herpetiformis (DH): An intensely itchy, blistering skin rash often found on elbows, knees, or the scalp.
- Neurological Issues: Including migraines, peripheral neuropathy (tingling in hands/feet), and balance issues (ataxia).
- Bone and Joint Pain: Early-onset osteoporosis or osteopenia due to calcium and Vitamin D malabsorption.
- Reproductive Issues: Unexplained infertility, recurrent miscarriages, or delayed puberty.
The Path to a Proper Diagnosis
The average time to receive a Celiac diagnosis is six to ten years, largely because symptoms overlap with so many other conditions. A definitive diagnosis follows a specific protocol:
- Serology (Blood Tests): Doctors look for specific antibodies, primarily the Tissue Transglutaminase IgA (tTG-IgA). Crucial Note: You must be consuming gluten for these tests to be accurate. If you start a gluten free diet before testing, the body begins to heal, and the tests may return a “false negative.”
- Genetic Testing: Testing for HLA-DQ2 and HLA-DQ8 genes can rule out Celiac Disease. If you do not have these genes, it is virtually impossible to have Celiac. However, having the genes only indicates a predisposition, not an active disease.
- Endoscopy and Biopsy: The “Gold Standard.” A gastroenterologist uses a small camera to view the small intestine and take tiny tissue samples. A pathologist then grades the damage using the Marsh Classification system (Type 3 usually confirms Celiac).

Mastering the Gluten Free Lifestyle
Transitioning to a gluten free diet is more than just swapping bread; it is a total lifestyle overhaul. It requires becoming a “label detective.”
The Big Three: Wheat, Barley, and Rye
Gluten is found in obvious places like pasta, cereal, and beer, but it is also hidden in:
- Sauces and Seasonings: Soy sauce (unless tamari), malt vinegar, and many salad dressings.
- Processed Meats: Sausages and deli meats often use wheat as a filler.
- Soups: Flour is a common thickening agent in canned or restaurant soups.
- Cosmetics and Medications: Lip balms, toothpastes, and vitamin fillers can contain gluten. While gluten must be ingested to cause damage, the risk of accidental ingestion from these products is high.
The Danger of Cross-Contact
For those with Celiac Disease, “just a little bit” is not okay. As little as 20 parts per million (ppm), roughly the size of a tiny breadcrumb, is enough to trigger an autoimmune response. This makes cross-contact (often called cross-contamination) a significant threat.
Creating a Safe Kitchen:
- Dedicated Toasters: Gluten free bread should never go in a shared toaster.
- Wooden Utensils and Cutting Boards: These are porous and can trap gluten particles even after washing.
- Colanders and Flour: Sifting flour creates airborne particles that can stay in the air for hours and land on safe surfaces.
- Shared Condiments: Double-dipping a knife from regular bread into the peanut butter or jam ruins the jar for someone with Celiac.
Social and Emotional Health
The psychological impact of Celiac Disease is profound. “Social anxiety” regarding dining out or attending parties is common. The fear of being “glutened” can lead to isolation. It is important to remember that Celiac is a manageable condition, not a limitation on joy.
Tips for Thriving:
- Advocate for Yourself: When dining out, speak directly to the chef or manager. Don’t just rely on a “GF” symbol on the menu.
- Bring a Dish: When attending events, offer to bring a safe, delicious dish so you know you have something to eat.
- Find Community: Support groups and online advocates provide a wealth of knowledge on safe brands and restaurant recommendations.
Long-Term Health and Monitoring
Once diagnosed, the journey doesn’t end with a gluten free diet. Regular follow-ups are necessary to ensure the gut is healing and to monitor for associated conditions.
- Nutrient Checks: Regular blood work for iron, B12, Vitamin D, and folate.
- Bone Density Scans (DEXA): Especially for those diagnosed later in life.
- Screening for Other Autoimmune Conditions: There is a higher risk of developing Type 1 Diabetes or autoimmune thyroid disease.
While there is currently no cure, research is ongoing into enzymes that may help digest trace gluten and vaccines to desensitize the immune system. For now, a strict, vibrant gluten free diet remains the foundation of health.
Frequently Asked Questions
No. Celiac Disease is a lifelong genetic autoimmune condition. While symptoms may fluctuate, the body will always react to gluten with an autoimmune response.
Celiac Disease is an autoimmune response that causes intestinal damage and long-term health risks. Non-Celiac Gluten Sensitivity (NCGS) causes similar symptoms but does not involve the same autoimmune mechanism or intestinal damage.
No. A product can be wheat-free but still contain barley or rye, both of which contain gluten.
Healing time varies. Children often heal within months, while adults may take two years or more of a strict gluten free diet for the villi to fully recover.
Standard oats are often cross-contaminated in the field or during processing. You must look for “Certified Gluten Free” oats.
It may be due to accidental cross-contact, hidden gluten, or secondary issues like lactose intolerance or Small Intestinal Bacterial Overgrowth (SIBO), which are common in Celiac Disease patients.
While a 100% gluten free home is safest, many families manage with a “shared” kitchen by using dedicated toasters, separate cutting boards, and strict cleaning protocols.
Yes. If you have a first-degree relative (parent, sibling, child) with Celiac, you have a 1 in 10 chance of developing it.
Yes. Anxiety, depression, and irritability are frequently reported symptoms, often linked to both the physical inflammation and the lifestyle stress of the diagnosis.
Gluten is too large a molecule to be absorbed through the skin. However, products used near the mouth (lipstick, toothpaste) or on the hands (lotions) pose a risk of accidental ingestion.
This is a rare form of the disease where the gut does not heal even after a strict gluten free diet. It requires specialized medical management.